An Overview of Cervical Degenerative Kyphosis
The cervical spine in its normal relaxed position aligns in a curved orientation called a lordosis. This is a “C” shaped curve with the opening of the curve toward the back of the neck. (See the second image). The reason for this curve’s existence is due to the angles of the base of the skull and top of the thoracic spine.
The head is required to be parallel to the horizontal for the eyes to be level. The base of the skull called the occiput is the location where the top of the spine connects to the skull. This area of the skull is tilted backwards about 30 degrees. The top of the spine has to match this angulation.
The lowest vertebra of the cervical spine meets the top of the thoracic spine. The top of the thoracic spine is typically tilted down to the front by about 10 degrees. This means that the neck has to have a curve (called a lordosis) of about 40 degrees to match the tilt of the skull and the base of the spine have the head level and the eyes to face the horizon.
The vertebrae are generally cylindrically shaped and have a slight forward slope due to the facets in the rear of the neck. Stacking the cervical vertebra on top of each other without the presence of the discs would create a forward tilted column. This curve is called a kyphosis-the reverse of the normal lordosis. It is the presence of the trapezoidal shaped discs that are thicker in the front than the back that creates the normal backwards curve (the lordosis).
Unfortunately, discs do degenerate. This degeneration can cause loss of the normal disc height. If the disc becomes severely degenerated, a localized forward angulation of a portion of the neck (a kyphosis) can occur. One degenerative level generally will not cause a real loss of the normal lordosis but two adjacent degenerative discs can. This reversal of the normal lordosis is called a cervical degenerative kyphosis. The change in angulation can create multiple problems.
It must be noted that the presence of these degenerative changes can cause no symptoms whatsoever. The third and fourth pictures attached here note a patient with the beginnings of degenerative kyphosis and this patient has no symptoms.
Pain Generation Due to Cervical Degenerative Kyphosis
Even though some patients have cervical degenerative kyphosis without symptoms, neck pain is a typical complaint noted with this disorder. Many different pain generators can cause neck pain.
Most neck pain is generated by the degeneration of the disc itself. When a disc degenerates, it loses shock absorption. Due to the abnormal curve, the forward angle of the degenerative kyphosis increases the load on the front of the vertebra where these degenerative discs are located.
Impact activities will increase the stress on these degenerative discs and increase pain. See the section on isolated disc resorption to understand how neck pain can be created by one degenerative disc. In the case of degenerative kyphosis, there are at least two and sometimes many more degenerative discs.
Eye-Righting Reflex
There is a reflex built into all humans called the “eye-leveling” or “eye-righting” reflex. This reflex causes us to keep our eyes level with the horizon. Normally, this position is quite easy to maintain as the normal relaxed position in a typical neck with an intact lordotic curve allows us to hold the head level.
In the presence of cervical degenerative kyphosis, the relaxed position of the head and neck will normally align the eyes to face the ground. In the presence of a degenerative kyphosis, holding the eyes level with the horizon requires hyperextension or extreme backwards bending of the neck. This requires constant muscle contraction to “pull” the head backwards to keep the eyes level.
To understand this effort, the equivalent would be to look up holding your head facing the heavens for most of the day. This position requires three dynamics that can cause pain.
First, the normal facets remaining in the neck have to slide on each other to increase the angulation. This prolonged bending backwards increases pressure on the facet surfaces and stretches the facet capsules. Facet overload pain can occur and possibly frank wearing out of the facets can occur..
The second problem is that holding the vertebrae in extension to compensate for the abnormal angulation of the degenerative vertebra requires significant prolonged muscle contraction. Over a long day, “holding the head up” produces muscle fatigue and a dull burning pain in the muscle belly of the extensor muscles.
The third problem has to do with the eye-leveling reflex itself. After a while, it takes so much energy to hold the head up that muscle pain occurs as noted above. Dropping the head relieves this muscle overload pain but then the eye visual alignment is positioned downward. Correcting this malposition requires holding an upward gaze to continue to do whatever work needs to be performed. This requires constant contraction of the eye elevator muscles. Eyestrain can develop and occasionally headaches will occur.
Other Problems Associated With Cervical Degenerative Kyphosis
Nerve root compression secondary to the degenerative changes can occur. See the section under cervical radiculopathy to understand this condition of foraminal stenosis. The extension of the neck required to accommodate cervical degenerative kyphosis can aggravate foraminal stenosis and cause nerve pain (shoulder and arm pain).
The angulation or slope of the vertebra due to degenerative kyphosis will increase the pressure on the facets. These facets can and do wear out. A pair of worn facets will lose stability and allow the vertebra above to slip forward on the vertebra below. This is called a degenerative spondylolisthesis and can cause instability as well as neck pain. See the last image in this topic to understand what this disorder looks like.
Loss of range of motion will occur with degenerative kyphosis. Normally, patients do not have significant complaints with this symptom but some are impaired.
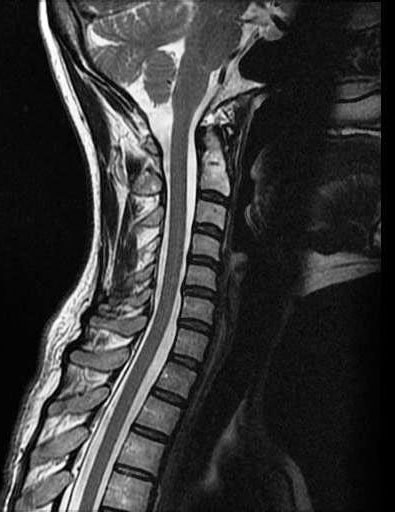
(Click to Enlarge Image) Normal Cervical MRI. Note that the neck does not have a normal curve due to the MRI image taken with the patient lying down.
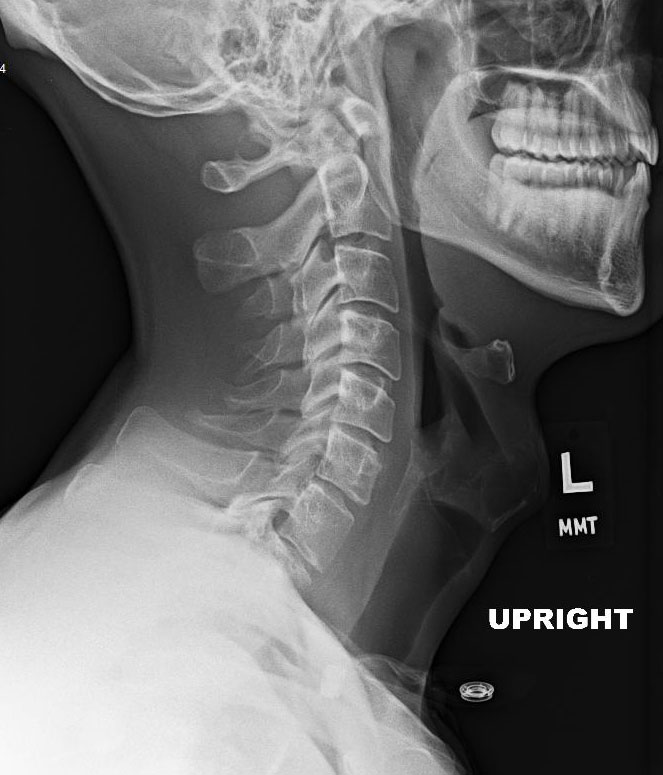
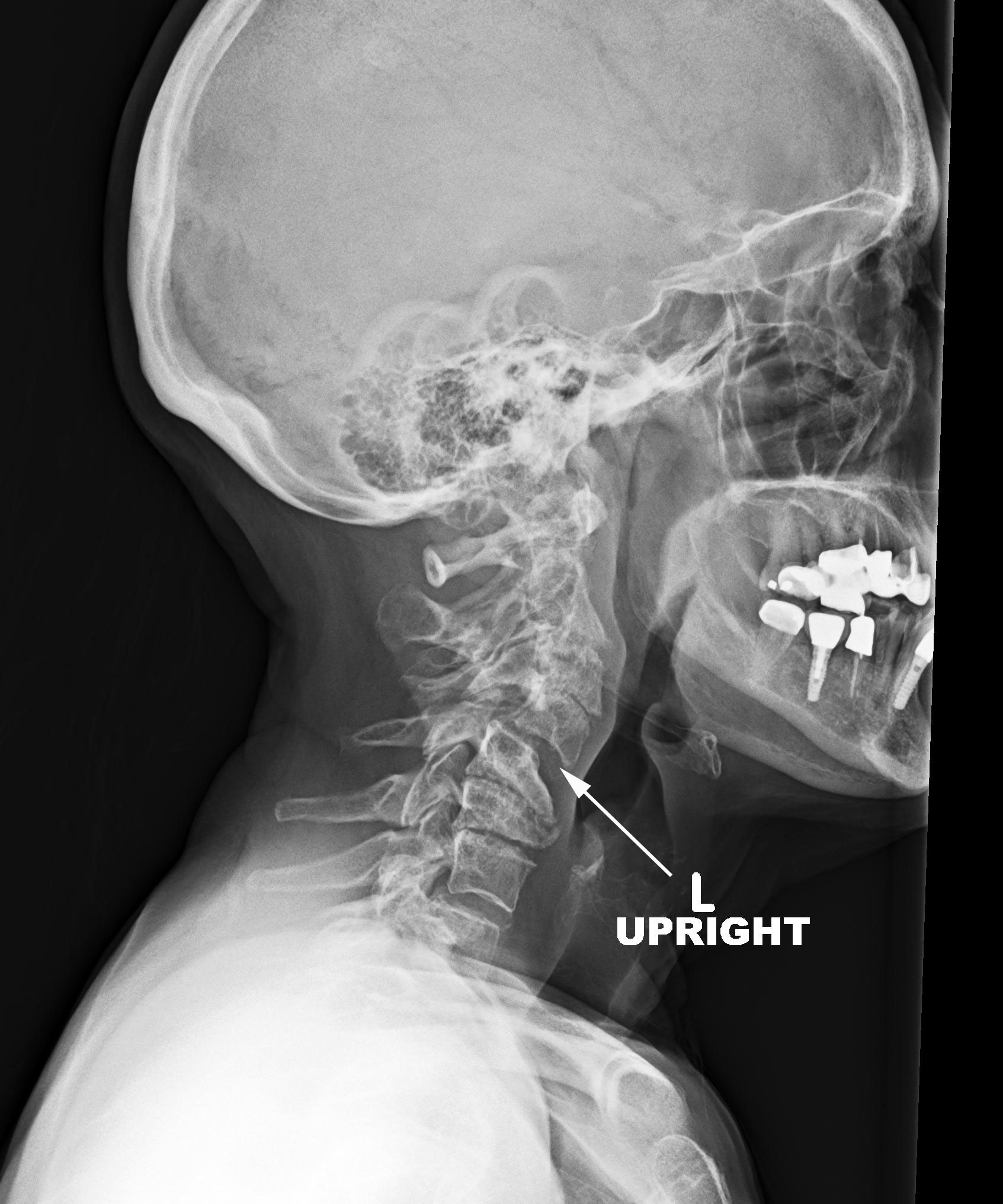
(Click to Enlarge Image) Normal cervical X-ray. Note the lordosis or curve of the neck is facing away from the face.
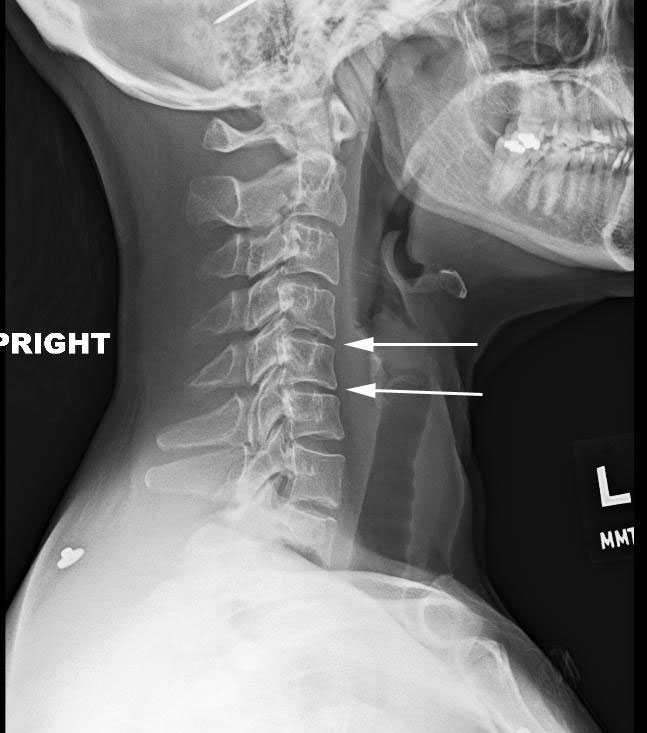
(Click to Enlarge Image) Early kyphosis (curve reversal) development. Arrows point to the two segments that are developing kyphosis.
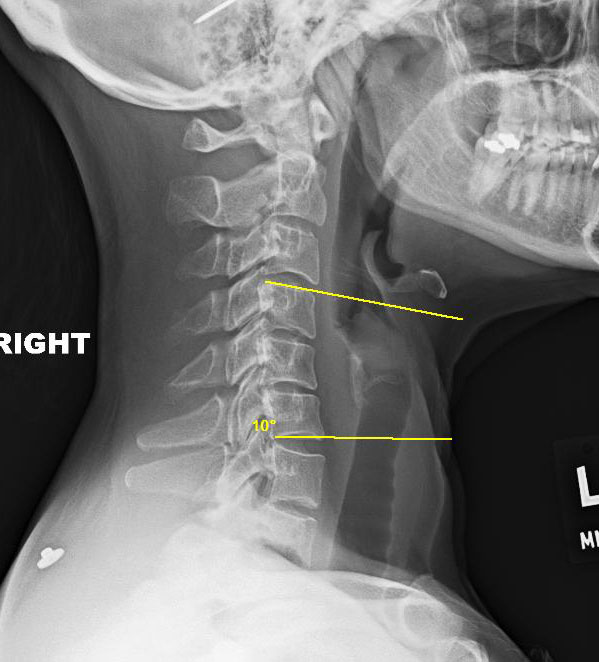
(Click to Enlarge Image) Early kyphosis development. The yellow lines are on the edges of the two vertebra. These lines should diverge (spread apart in front) but instead converge due to the kyphosis.
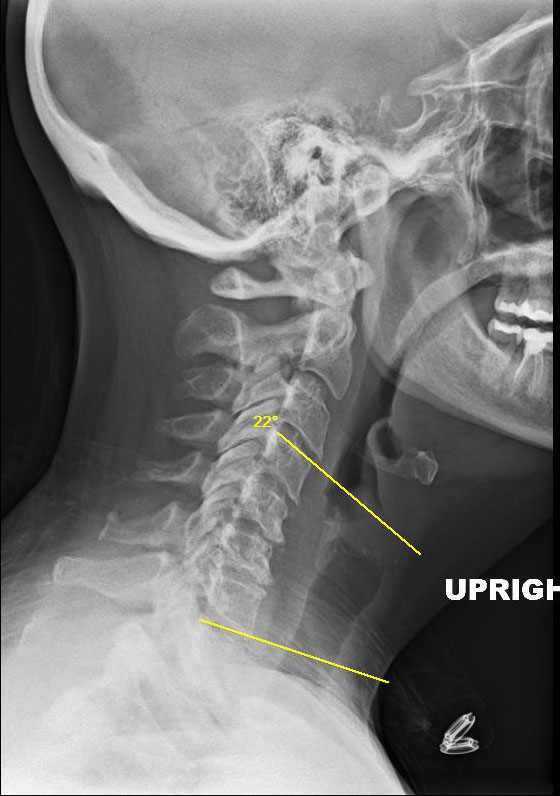
(Click to Enlarge Image) Neutral X-ray of degenerative kyphosis. The yellow lines note a 22 degree kyphosis. Patient has failed all non-operative care and is miserable.
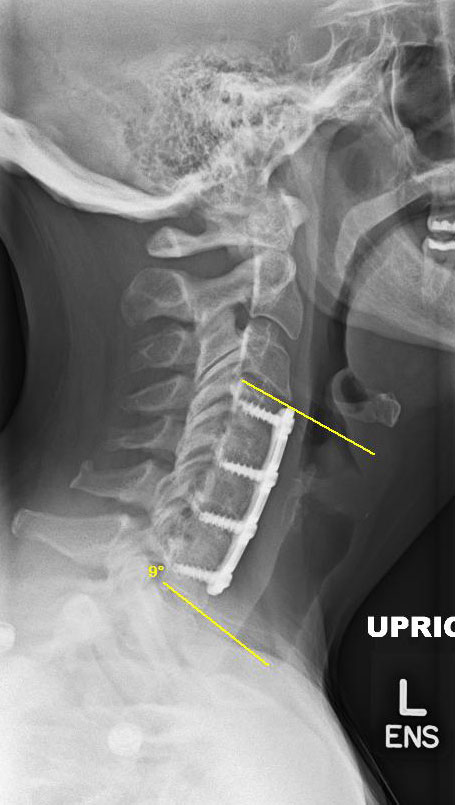
(Click to Enlarge Image). After surgical correction. Note the yellow lines diverge in-front indicating a lordosis has been reinstituted. The lordosis is now 9 degrees.
(Click to Enlarge Image) Severe degenerative kyphosis. In this case, the kyphosis has worn out the facets above at C4-5 (arrow) allowing a degenerative slip.
Are you suffering from symptoms of Cervical Degenerative Kyphosis?
Would you like to consult with Dr. Corenman about your condition?
You can set up a long distance consultation to discuss your
current X-rays and/or MRIs for a clinical case review.
(Please keep reading below for more information on this condition.)
Treatment of Cervical Degenerative Kyphosis
Diagnosis of this disorder by a physician is not difficult. The standard side view (sagittal) X-ray in the standing position with the neck relaxed will reveal degenerative kyphosis. Interestingly, the MRI and CT scan are less capable of looking at alignment as both of these studies are performed lying down where the effects of gravity are negated. Patients may have neck pain, muscle fatigue, eyestrain and headaches secondary to degenerative kyphosis.
To repeat, the presence of degenerative kyphosis without symptoms needs not be treated. If symptoms are disturbing, treatment should be started. Initially, conservative treatment needs to be employed. Physical therapy, medications, activity restriction and ergonomics need to be engaged. Many patients will have reasonable relief or at least pain management with these measures.
For patients who do not respond to conservative measures, surgery can be considered. The goal is to realign the neck into lordosis to reduce the pressure on the normal bordering segments and to decompress the nerves and spinal cord. Normally, due to the severe degeneration of the discs, a fusion (ACDF) is employed.
To learn more about cervical degenerative kyphosis and treatment options, please contact the practice of Dr. Donald Corenman, spine specialist and neck doctor offering diagnostic and surgical second opinions to patients in the USA and around the world.
Related Content
- Cervical Degenerative Spondylolisthesis
- Cervical Central Stenosis & Myelopathy
- Chronic Radiculopathy
- Cervical Degenerative Disc Disease
- Cervical Degenerative Facet Disease
- Cervical Spine Instability
- How to Describe Your History and Symptoms of Neck, Shoulder and Arm Pain
- Best Questions to Ask When Interviewing a Spine Surgeon or Neurosurgeon
- When to Have Neck Surgery