Anatomy of the Joints and Cervical Degenerative Spondylolisthesis Overview
In either the cervical or lumbar spine, the paired facets in the back of the spine are the great stabilizers of the vertebral column. The facets are lined up like shingles on a roof, interlocking the superior segment of the vertebra above to the back of the inferior segment below.
This alignment allows these joints to act as “railroad tracks”. The facets guide the movement of the vertebra to allow certain motions (bending forward and backwards, lateral bending) and prevent detrimental motions (shear and lateral translation). Shear is a shifting of one vertebra on the one below in the forward or sideward direction.
The disc, which is sandwiched in between the two vertebral bodies does not by itself have the capability to prevent a shift or slide. The disc has very little resistance to shear. In fact, shear forces are a common cause of disc tears (annular tears).
The facet joints provide the mechanical locking that prevents the vertebra above from sliding forward on the vertebra below. Shear forces or slips (forward or lateral) cannot occur if these joints are “doing their job”. That is why I call the facets the “doorstops” of the spine. If a forward slip or shift of the upper on the lower vertebra occurs, it is due to the wearing out of these joints, called an “anterolisthesis” or “degenerative spondylolisthesis”.
These facet joints are normal joints just like the knee, hip or shoulder joints and there are more joints in the spine than all the others in the body combined. These joints (called diarthrodial joints) are made up of two opposing smooth bony surfaces each coated with hyaline cartilage. Hyaline cartilage is a firm but slippery material that has some “give” to it. The consistency is somewhat like a soft plastic.
These facet joints are united together by a strong sheet of collagen called a capsule made of material similar to burlap. The capsule attaches to the periphery of these joints and surrounds them like a bag over the joint. This capsule prevents excessive motion. The facet joint is lubricated by the synovial fluid, a thin and slippery fluid made by the synovium, which lines the inside of the joint. This fluid turns into a film that makes the two cartilage surfaces very slippery.
The joint surfaces are so perfectly matched and smooth that with the synovial fluid, there is a strong vacuum that holds the joints together. Breaking this vacuum produces a popping sound similar to removing a wet glass from a smooth counter. In general, there is no danger in breaking this vacuum and it can feel quite good, as when a Chiropractor manipulates the spine. However, in cervical degenerative spondylolisthesis, manipulation is contraindicated.
Even when these joints remain intact, they will not prevent a backwards slide (called a retrolisthesis). This backwards slide can occur when the facet capsule becomes stretched out but the facet structure (bone and cartilage) is still intact. The disc has to narrow (degenerate) to allow this backwards slide to occur.
Degeneration or Arthritis?
Arthritic changes can “wear’ these cartilaginous surfaces of the facet joint down. This can be in the form of erosions of the surface of the joint or joint mice (broken off pieces of cartilage) that “float” in the joint and can act like sand in engine oil and cause premature wear.
Many individuals reading this thread currently have mildly arthritic but non-symptomatic (non-painful) cervical joints. In fact, if you are in a very quiet room and listen intently, you will probably be able to hear faint grinding noises in the back of your neck when you turn your head side to side.
What is interesting is that a cervical degenerative spondylolisthesis tends to occur above and below very degenerative discs. That is, the discs below this slip level have become so degenerative that they are relatively immobile. This increases the stress on the facets above the degenerative disc levels and wears them out prematurely. See the accompanying image (image 3) to understand this concept.
When the cartilage wears down, there is direct bone-to-bone contact in this facet joint. This contact can wear down or erode the bone surfaces. When these bony surfaces erode, the joints no longer can hold the two vertebrae in perfect alignment and a slip occurs. With both sides worn down, a forward slip called a degenerative spondylolisthesis will occur. If only one joint is worn and the other side remains intact, a rotary listhesis will occur (a slip on the side of wear that rotates the vertebra above on the vertebra below).
Instability can occur with this forward slip. Instability is the inability of the two vertebral segments to maintain normal alignment when exposed to the normal day to day forces that the neck is typically subject to. Instability can cause local neck pain and endanger the nerve roots or spinal cord.
The forward slip of the upper vertebra on the lower one has ramifications for the diameter of the spinal canal. Since the canal is a series of concentric rings piled perfectly one on top of another, the forward slide of the upper vertebra can significantly narrow the canal and potentially compress the spinal cord.
Because the volume of the canal, with or without this pinching will enlarge with forward bending and decrease in size with backward bending, you can imagine what happens to the canal that is already narrowed when you add backwards bending. This narrowing of the canal can cause compression of the cord and a condition called myelopathy-dysfunction of the spinal cord. See this website for a description of these symptoms.
With the presence of this narrowing, an impact onto the front of the head can cause a more significant compression of the cord called a central cord syndrome. See the website for further details of this injury.
The erosion of these joints also causes increased bone spur production as the bone tries to compensate for instability by increasing its surface area. Of course, these bone spurs “don’t care” where they grow. Ingrowth into areas that are quire sensitive such as the nerve root exit holes (the foramen) and the central spinal canal where the spinal cord lives is not uncommon.
Related Content
- How to Describe Your History and Symptoms of Neck, Shoulder and Arm Pain
- Best Questions to Ask When Interviewing a Spine Surgeon or Neurosurgeon
- When to Have Neck Surgery
- Chronic Radiculopathy
- Cervical Degenerative Disc Disease
- Cervical Spine Instability
- Cervical Spine Fractures and Dislocations
- Cervical Radiculopathy or Pinched Nerve in the Neck
- Cervical Herniated Disc
- Arthritis of the Neck and Back
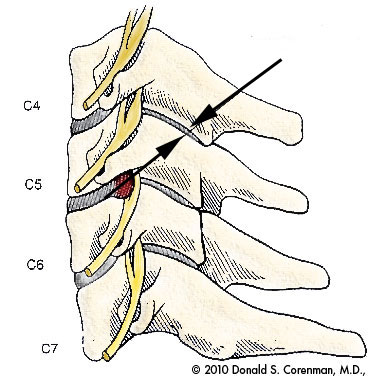
Black arrows point to cervical facet. Note that the facet is angled to ‘hook’ the back of the vertebra together. When intact, this hook acts like a ‘doorstop’ to prevent the vertebra above from sliding forward on the vertebra below.

Degenerative spondylolisthesis (arrow). Note the significant narrowing of the discs below the slip level. You cannot ‘see’ the facets on this image as this is a midline cut and the facets are not found in the midline.
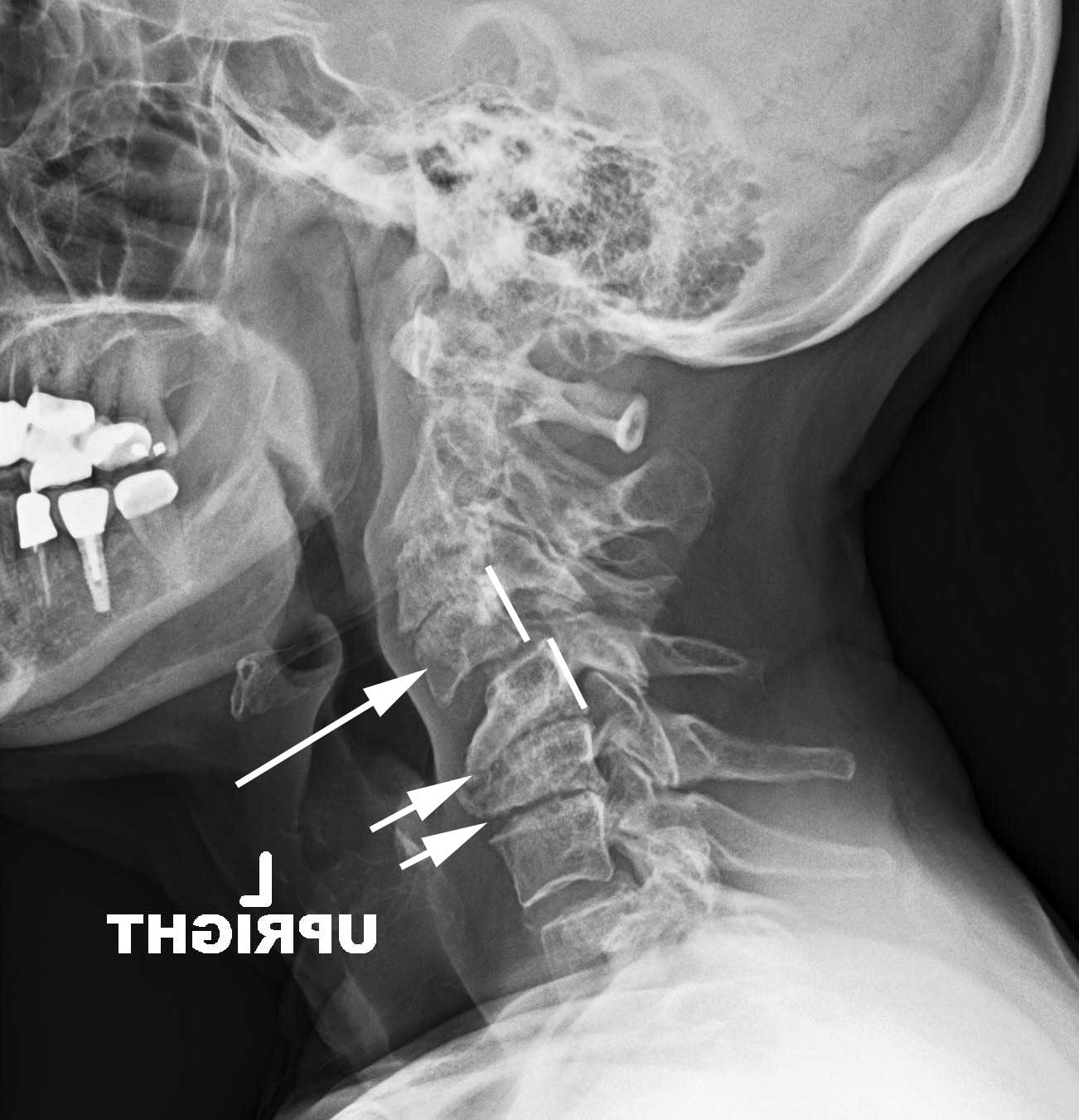
Typical degenerative spondylolisthesis in the cervical spine. Small arrows point to the very degenerative discs below the slipped level. The larger arrow points to the slip of C4 on C5.

Instability. Note that with flexion (bending forward), C4 moves forward on C5. The motion puts the cord in jeopardy.

Stenosis (narrowing) of the spinal canal in a degenerative spondylolisthesis. The arrow points to the slip level and the cord compression. The two lines indicate the back of C4 and C5. The two lines normally should align evenly.

Degenerativ spondylolisthesis with cord injury. Large arrow points to slip level. Small arrow points to the cord injury where the slipped C6 vertebra impacted into the spinal cord. There is signal change of the cord (whiter area) indicating injury.
Are you suffering from symptoms of Cervical Degenerative Spondylolisthesis?
Would you like to consult with Dr. Corenman about your condition?
You can set up a long distance consultation to discuss your
current X-rays and/or MRIs for a clinical case review.
(Please keep reading below for more information on this condition.)
Symptoms of Cervical Degenerative Spondylolisthesis
The most common symptom of a cervical degenerative spondylolisthesis is neck pain. With instability, painful popping and clicking and back of the neck pain can occur. However this condition may be present and painless. This painless condition can be a problem occasionally as rarely, a catastrophic injury may occur based upon a fall onto the head or neck and injure the nerve root or spinal cord. Myelopathy can occur and its symptoms are well documented under the myelopathy category on this website. Shoulder and arm pain can occur when the nerve root is compressed.
Treatment of Cervical Degenerative Spondylolisthesis
Non-Surgical
Treatment for cervical degenerative spondylolisthesis is based upon the symptoms, the amount of compression of the cord and nerve roots and the instability present. In many cases, if there are no symptoms, and no threat to the cord, there is no need for treatment. If the patient has actual neck pain from the facet arthritis, physical therapy, chiropractic, medications, activity avoidance and facet injections can be helpful.
Chiropractic treatment (manipulation) is contraindicated if there is instability or a slip that creates compression of the cord and possibly nerve roots.
If facet injections help but last only temporarily, dorsal facet rhizotomies can be effective (see website). A rhizotomy is an outpatient procedure that attempts to desensitize the facet by burning the small sensory nerves that supply this joint. Its effectiveness in the right setting is about 70% but may have to be repeated in one year as the sensory nerves attempt to grow back.
Surgical
Surgical correction of cervical degenerative spondylolisthesis can be important. If there is instability, cord compression, symptomatic nerve compression or significant neck pain, the proper surgery to correct this condition is an ACDF (anterior decompression and fusion- see website). This procedure will realign the two vertebrae and lock them in place to prevent cord and root injury as well as prevent the painful motion that accompanies this disorder.
There are two surgeries that are contraindicated in the presence of this slip; foraminal decompression (a hemilaminotomy/posterior foraminotomy) or an artificial disc replacement (ADR). The vertebrae are already slipped on each other due to the failure or erosion of these facets. A foraminotomy removes even more bone from the facet to open the nerve hole (foramen). This additional bone removal will further increase the already unstable slip.
The artificial disc requires normal and intact facets for proper mechanics. Replacing the degenerative disc with a more mobile surface (the ADR) will increase the load on the facets, which are incompetent in this disorder. This will allow greater stress to be placed on the artificial disc components and cause premature wear.
For more resources on cervical degenerative spondylolisthesis, or to discuss treatment options, please contact Dr. Donald Corenman, spine specialist and neck doctor offering diagnostic and surgical second opinions to patients in the USA and around the world.