Cervical Radiculopathy Overview
Cervical radiculopathy (also referred to as a pinched nerve in the neck) is a condition where the nerve root in the neck is compressed either by a herniated disc or by a bone spur. If a compressed nerve in the neck is caused by a herniation, please see the section on cervical herniated disc for a complete description. Many individuals sometimes refer to a compressed nerve as a “pinched nerve in the neck”. These are common reasons for ongoing neck pain.
The cause of this nerve compression lies with the design of the uncovertebral joint. As noted in the anatomy section, this joint is not present in the infant and slowly develops with maturity. The reason this joint develops lies with the design of the surfaces of the vertebral body.
Instead of having flat parallel surfaces that the disc attaches to (like the thoracic and lumbar vertebra), the sides of the body of the cervical vertebra are sloped upwards like a smile when viewed from the front. The disc is wedged in between the two vertebral bodies. Over time, the two surfaces of the vertebral bodies touch. Since they are lined with cartilage, they form an articulation-essentially a new joint!
The disc in many people becomes degenerative over time. Degenerative discs of the cervical spine are causes from aging, wear and tear, and injury. Discs become degenerative because a disc has no blood supply after the age of eight and can’t repair itself when injured. The central nucleus (the jelly in the donut) will eventually lose pressure. Just like letting air out of a car tire, the disc loses height. With this height loss, the two vertebral bodies approximate or come closer together. The uncovertebral joint sitting on each side of the disc space undergoes increased pressure and simply wear out.
The uncovertebral joint-like any other joint will develop bone spurs with this undue pressure. Since this joint makes up the front wall of the foramen or hole that the nerve exits, this bone spur can crowd out the nerve root that sits immediately behind the spur. If the nerve root becomes pinched it will swell which obviously compounds the problem. A swollen root won’t fit well into an already narrowed exit hole.
Biomechanics
The biomechanics of ICD radiculopathy/cervical radiculopathy (pinched nerve in the neck) are easy to understand. The nerve hole itself becomes larger with bending forward and away from the side that it is on. Bending the head backwards or to the side that the nerve hole or foramen is on will narrow this hole. Therefore, with this condition, arm and shoulder pain will normally become worse with bending the head backwards or bending the head to the side of the arm pain. Obviously avoid any head motions that increase the pain into the arm, as it is not a good idea to crush this nerve any further.
Cervical Radiculopathy Symptoms
Compression of one of the neck nerves normally causes shoulder and arm pain. There are many patients that have pain that also radiates to the area between the shoulders and this symptom is commonly misdiagnosed as thoracic or scapular (shoulder blade) pain when it is really referral pain from the compressed nerve
If the compression is more severe, not only pain and numbness can occur but also the muscles attached to the nerve can become weak. For example, if the C6 nerve is significantly compressed, the individual will have weakness of the biceps (the upper arm muscle that lifts a weight such as a suitcase) and the wrist extensor (weakness causes difficulty with holding objects).
Certain sports will make the pain worse because of neck positioning. Both swimming and cycling require neck extension and will typically aggravate this pain. Other sports have components of extension inherent, which will also cause momentary shoulder and arm pain. The follow through in the golf swing and the serve in tennis require momentary neck extension that can cause a “jolt” of pain during the maneuver. Volleyball and bowling are among many other sports that will also cause this pain.
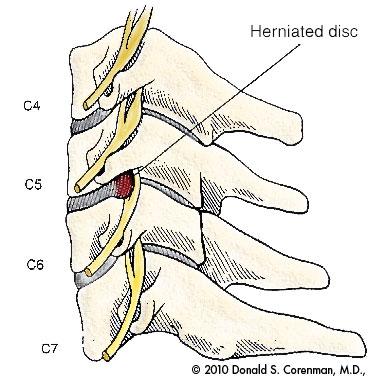
(Click to Enlarge Image) This illustration is a side view of the cervical spine (neck). Here you can see the vertebral bodies with the discs in the front of the spine and the facets in the rear. The nerve roots exit through the sides of the spine.
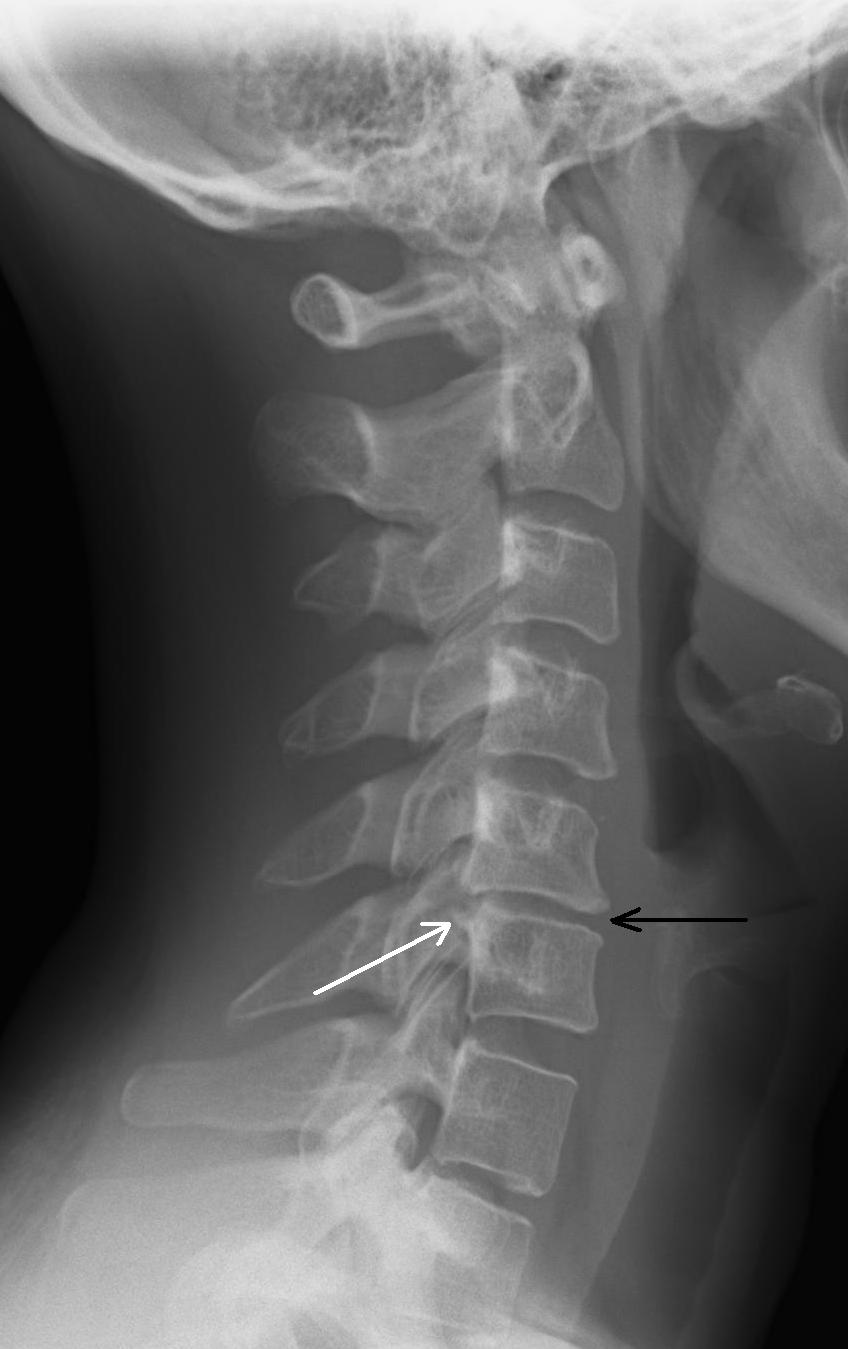
(Click to Enlarge Image) This is a side view of a cervical spine (neck) with a degenerative disc at C5-6. The black arrow points to the narrowed disc and the white arrow points to the bone spur projecting off the back of the disc into the spinal canal.
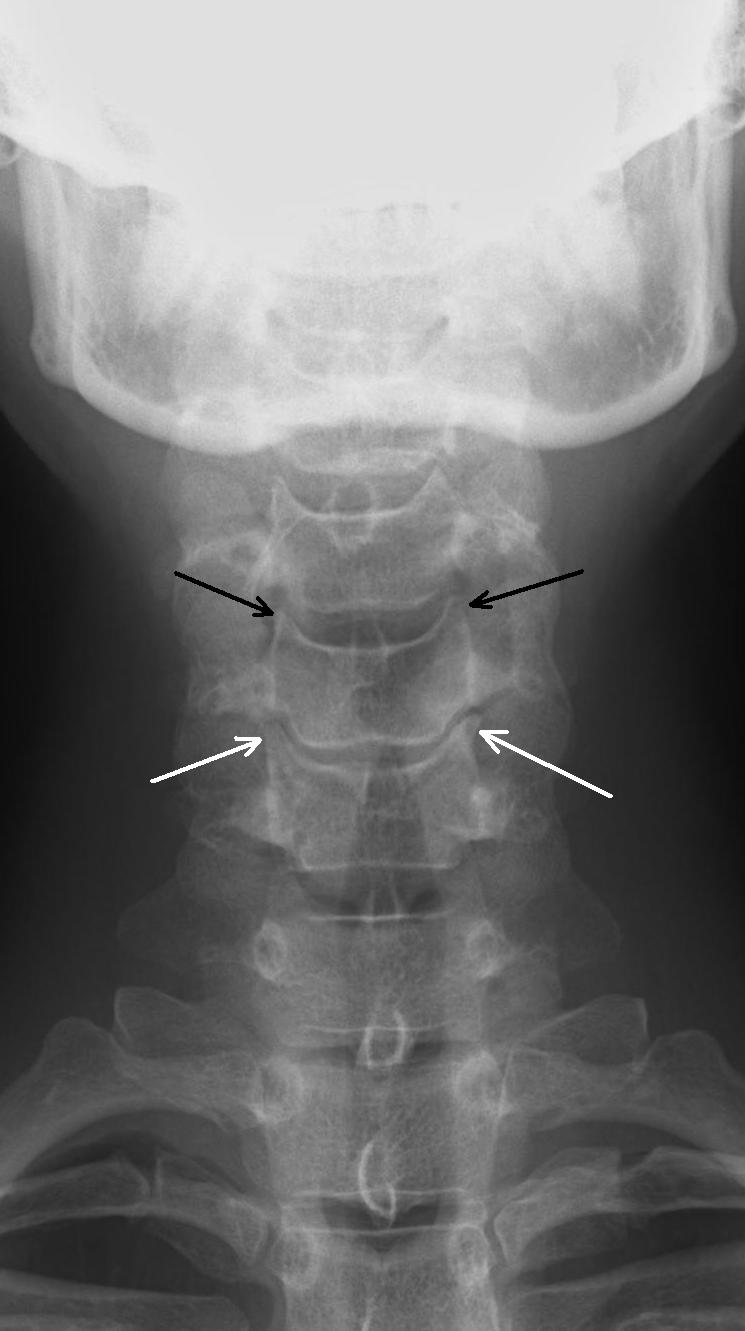
(Click to Enlarge Image) This is a front to back view of a cervical spine (neck) X-ray. The black arrows point to the small pyramid shaped normal uncovertebral joints and the white arrows point to the degenerative uncovertebral joints. Compare the normal to the abnormal to see the enlargement of these joints with a “mushroom head” on one.

(Click to Enlarge Image) This is a side view picture of a patient who had significant compression of his C5 nerve for a period of time. You can see the “hollowing out” of the back of his shoulder where the deltoid muscle has undergone significant atrophy.
Cervical Radiculopathy Treatment
Non-Surgical
Non-surgical treatment of cervical radiculopathy (pinched nerve in neck) includes medication, injections to reduce the swelling and irritability of the nerve root and a physical therapy program to strengthen the muscles that surround the neck.
Surgical
For bone spurs that compress the nerve, there are surgeries of the spine to help and there are two surgical treatments that are generally effective; an anterior cervical decompression and fusion (ACDF) or an artificial disc replacement (ADR). If the disc is too degenerative, an ADR would not work. Posterior cervical foramenotomy generally is not indicated in this disorder as the spur is not accessible by this approach. It’s important to understand all of the risks of spine surgery.
If you live in the Vail, Aspen, Denver and Grand Junction, Colorado communities and would like more information on cervical radiculopathy, please contact Dr. Donald Corenman, spine specialist and neck doctor.