Rotator Cuff Syndrome as a Cause of Neck Pain
The shoulder joint is very different from every other joint. The shoulder joint (also known as the glenohumeral joint) has the greatest range of motion in the human body due to its design. This design also creates stresses to the shoulder that makes it more vulnerable to injury.
In comparison to the hip, the shoulder is much less stable. Where the hip has a large bony ball (the femoral head) and surrounding deep bony socket to cradle that ball, the shoulder has a very large ball (the humeral head) but a very shallow socket (the glenoid cavity) .
This design allows enormous range of motion of the shoulder joint. There is little however in the bony structure of the shoulder to “keep it in place”. One of the structures that help to hold the large shoulder ball in the shallow socket is a soft tissue extension of the socket called the labrum. The labrum “deepens” the shoulder socket to help with stability.
The main reason the shoulder is stable in so many different positions however is a group of four muscles together called the rotator cuff. These muscles originate from the front of the chest, the top and the back of the shoulder blade. They surround and envelope the shoulder joint to hold the ball into the socket.
These muscles “hold” the shoulder in place by muscle contraction. They literally pull the ball into the socket. In addition, these muscles assist with rotating the arm to the front and the back (the very reason they are called the “rotator cuff”). These four muscles blend into a tendon called the rotator cuff tendon which is a thick but flat tendon that inserts into the humerus-the upper arm bone.
The muscles (the subscapularis, supraspinatus, infraspinatus and teres minor) travel through a bony tunnel below the top of the scapula (the shoulder blade) capped by an overhanging bone called the acromion. You can feel this bone with your fingers as it is right under the skin. The collar bone (clavicle) also insets into the acromion, which can be felt in the front of the shoulder.
The tip of this acromion can develop a bony spur, a small elongation of the end of this bone. The acromion can also develop a small “hook” called a type II or type III acromion which predisposes the shoulder to rotator cuff tears.
This spur or hook can dig into the rotator cuff tendon when the arm is lifted overhead. This constant “digging in” (called an impingement) can wear out the rotator cuff tendon leading to tendonitis and bursitis. A through and through tear of the tendon can eventually occur. This is especially noted with repeated activities of shoulder elevation but can happen to sedentary individuals too.
Rotator cuff pain is common in both middle aged and elderly patients as well as young athletes. Younger athletes who participate in overhead sports such as swimming, baseball pitching, and tennis are the most vulnerable. Workers who use repetitive lifting or overhead activities such as wallpapering, construction, or painting are also prone to this injury. Pain may also occur as the result of a minor injury such as a fall onto an outstretched arm.
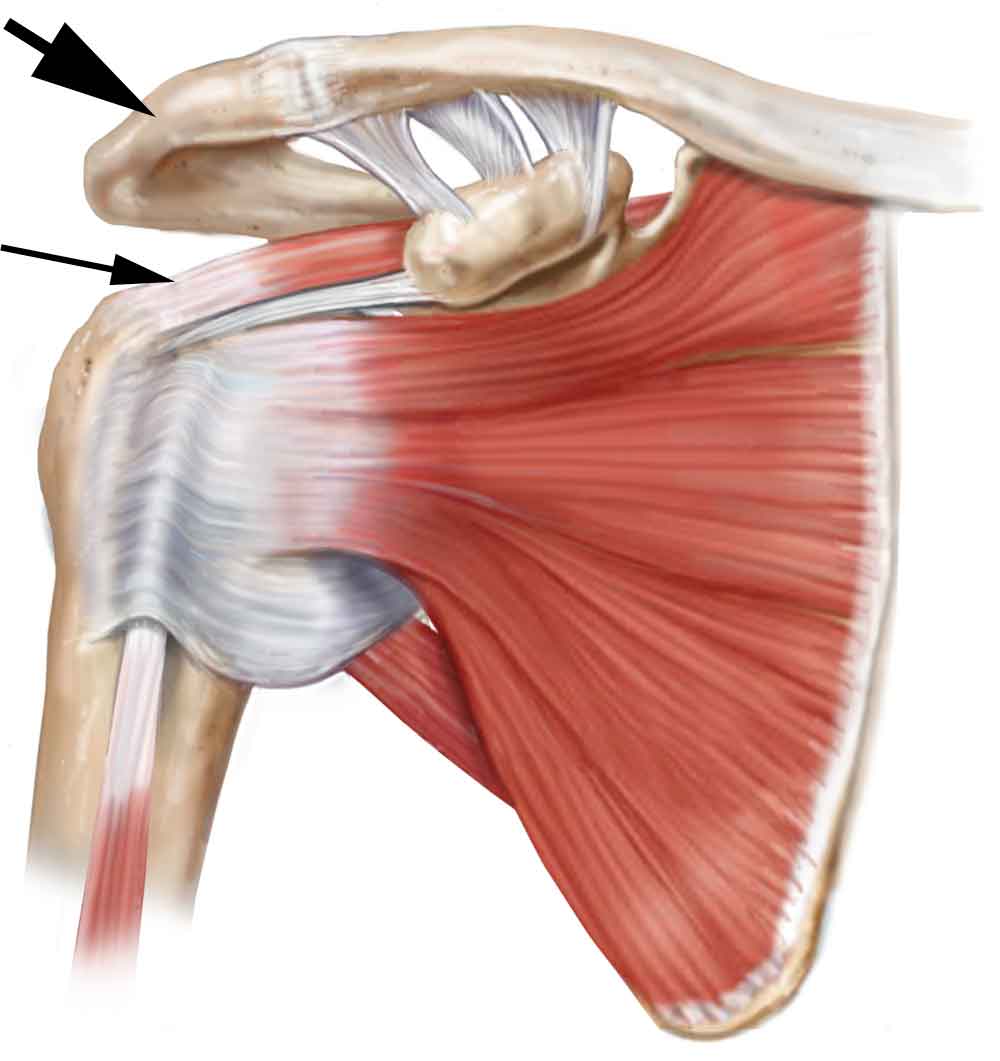
(Click to Enlarge) Shoulder and rotator cuff. Thick arrow points to acrominium and smaller arrow points to rotator cuff tendon.
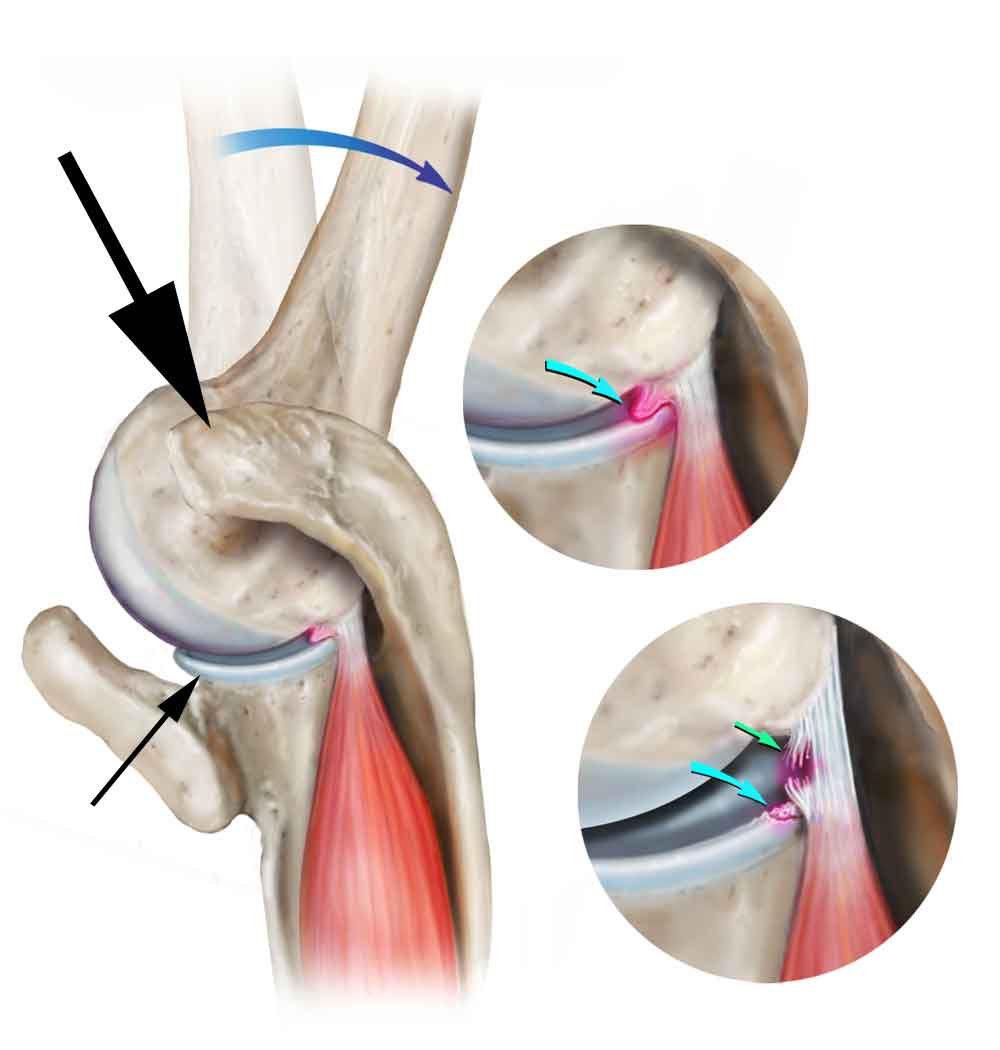
(Click to Enlarge) Top down view of impingement. Large black arrow points to acrominium. Small black arrow to shoulder joint.
Are you suffering from neck pain associated with rotator cuff syndrome?
Would you like to consult with Dr. Corenman about your condition?
You can set up a long distance consultation to discuss your
current X-rays and/or MRIs for a clinical case review.
(Please keep reading below for more information on this condition.)
Symptoms of Rotator Cuff Syndrome
Rotator cuff impingement syndrome initially creates pain in the top of the shoulder with shoulder elevation such as lifting the arm over the head or reaching behind. This pain might occur with activities such as when cleaning the top of a cabinet or sleeping with the arm over the head. If this disorder progresses, the pain can be constant and the shoulder can ache even without movement. Commonly with advanced disease, pain can be constant and wake the patient up at night.
Typical activities such as reaching the arm behind to put on a coat or even driving by holding the upper part of the steering wheel can generate pain.
The pain can radiate up to the neck. The muscles of the rotator cuff do not insert into the neck but the secondary shoulder stabilizers do (levator scapulae and trapezius). These secondary stabilizers are overstressed due to the poor rotator cuff muscle strength. The pain can also radiate over the shoulder to the elbow region and rarely I have seen pain radiate below the elbow.
Weakness of the shoulder can occur with significant inflammation due to pain inhibition. Pain causing weakness occurs when contraction of the shoulder muscles places tension on the damaged and inflamed tendon. When the pain ensues, a neurological condition called reflex inhibition is triggered to prevent the patient from contracting the shoulder muscles and further damaging this tendon.
With continued impingement, a partial or complete tear of the rotator cuff tendon can occur. This creates a mechanical disruption of the tendon, which significantly weakens the rotator cuff. Many rotator cuff tear patients cannot lift up their arm.
Rotator Cuff Syndrome vs. Cervical Radiculopathy
Unfortunately, a pinched nerve in the neck (cervical radiculopathy) can mimic a rotator cuff impingement syndrome. Pain from a C5 nerve pinch or even C6 nerve compression will radiate pain into the shoulder and can weaken the shoulder muscles. This creates a diagnostic dilemma.
To differentiate between these two disorders, a careful history, physical examination, evaluation of the images (X-rays, MRI and others) and diagnostic injections are used.
The history can on occasion be confusing. Shoulder and neck patients both can have shoulder aching and neck aching. Typically, neck patients with arm pain will feel better with their arm up and shoulder patients gain some relief by holding their arm down at their side but this is not always the case.
Neck patients generally will not like to extend their head (bend backwards) where shoulder patients are not affected by neck extension. Shoulder patients generally have no paresthesias (pins and needles) in their shoulder and arm area whereas spine patients can display these symptoms. Pain can overpower the sensation of paresthesias however so neck patients may not know they have these symptoms.
Examination should note some subtle differences that can help clear up the confusion of the pain generation structure.
If there is any question, the gold standard for differential is a diagnostic injection. A selective nerve root block (SNRB) of the C5 or C6 nerve should give no shoulder relief if this is a true shoulder disorder. The neck injection should give temporary relief if the origin of pain is the nerve root (see pain diary). Likewise, a shoulder injection should give no relief if the disorder originates from the cervical spine but should give great relief if the shoulder is involved.
If you would like additional resources on rotator cuff syndrome as a cause of neck pain, please contact the office of Dr. Donald Corenman, neck doctor and spine specialist serving patients in the Vail, Aspen, Denver and Grand Junction, Colorado area.