What are Spinal Injections?
Injections in the cervical and lumbar spines have long been used to both diagnose and treat nerve irritation, canal stenosis and disc pain. These injections can be very helpful even in the long term to yield spine and extremity pain relief. Below, a detailed discussion is offered on epidural injections and selective nerve root blocks–diagnostic and therapeutic.
What is the difference between epidural steroid injections (ESI) and selective nerve root blocks (SNRB)?
The difference between epidural steroid injections (ESI) and selective nerve root blocks (SNRB) requires going back to anatomy. The dura is the membrane inside the spinal canal which makes up the long tube from the brain to the tailbone. This dural sac contains the nerves and the cerebrospinal fluid or CSF. The nerves then branch out from this sac like tree branches (one on each side) at every level to exit the spinal canal (see the anatomy section).
The Latin term “epi” means “above” so an epidural injection is an injection above the dura. This injection is normally placed around the center of the neck or back and the medication is deposited on top of the dura. The SNRB puts medication at the nerve root branch from the spine in the area called the foramen. With a small volume, only the exiting nerve root can be targeted. With a larger volume, the medication will enter the canal and cover more than one nerve root.
How Do You Choose Which One?
The choice of injection location depends upon the problem area suspected of causing pain. If the canal is stenotic (narrowed), a central injection or ESI would be used. If a nerve is suspected of causing pain, a SNRB would be used in the foramen that the nerve exits. Now to confuse the issue, you can introduce medication into the central canal through the foramen if you use enough volume. This would be called a trans-foraminal epidural steroid injection (TFESI). If disc pain is suspected, either route (ESI or TFESI) would be acceptable.
Diagnostic vs. Therapeutic
Epidural injections and selective nerve root blocks–diagnostic and therapeutic–which one to choose? There are two medications injected at the same time. One is a numbing agent and the other is a steroid. With both medications injected at the same time, the injection is called “diagnostic and therapeutic”. If just the numbing medication is injected, it would be called a diagnostic test. If only the steroid was injected- obviously the injection would be called a therapeutic injection.
The part of the test named “diagnostic” involves numbing the structure or structures thought to be involved in the pain generation. This can be a nerve root, a disc or the entire canal. This is just like a trip to the dentist. An injection into the jaw anesthetizes the sensory nerve and makes the jaw feel “numb and swollen”. After three hours, the feeling or sensation returns.
The same concept is used with the diagnostic injection into the structure thought to cause the pain. The first three hours after the injection will numb that area. If the region that is numbed is causing the symptoms, there should be relief of pain for about two to three hours while repeating the activity that causes pain (sitting, standing, walking bending or whatever action induces the pain). This of course means that if sedation is used during the injection-it must have worn off in a short period of time. If you are sedated for three hours and lie in the recovery room, the diagnostic portion of the injection will be lost and the injection will have to be repeated.
Pain Diary
The most important thing post injection is to get up and repeat the activity that causes the pain in the three hour diagnostic “golden window”. Do not just sit around after the injection! A pain diary needs to be kept both prior to the injection and after the injection. Please see the section on providing a pain diary to understand how to fill one out.
Steroids
The therapeutic portion of the injection is the steroid. The steroid medication is wonderful for nerve inflammation. Someone should develop a bumper sticker “Nerves Love Steroids”. These steroids are corticosteroids and not the anabolic type that body builders use to look like a puffed up balloon. The body manufactures about 8-10 mg/day of this in the adrenal glands.
There are multiple actions of steroids that benefit nerves. The main action of the steroid is to prevent the chemical cascade that causes inflammation. A cascade is an amplification system to get a small matter big attention. For example- a small inflammatory source (a cut or abrasion) will cause multiple amplifications in a cascade. The first step magnifies the response 100 times; the next step multiplies that step 100 more times and so on. There may be 7-8 steps for this cascade to continue. Breaking this cascade is the specialty of the steroid.
What the steroid prevents is swelling, breakdown and tissue destruction of the injured area (which is what inflammation really is). Normally the chemical cascade “calls” in white blood cells (WBCs) to do their work. When the white blood cells (WBCs) migrate to this area, they release their contents which cause more swelling and even some tissue destruction (normally designed to “clean up” the injured area but in this case, causes more nerve injury). Swelling occurs when the under the influence of the chemical mediators of inflammation- small blood vessel walls in the vicinity become more “leaky” and tissue fluid floods into the area. The WBCs literally dissolve and eat (phagocytize) the dead and dying tissue. This is great for healing a tendon or skin abrasion but not so good for the nerve root.
The steroid also seems to “toughen” the nerve root. The lack of swelling and irritation reduces the size of the herniation but also probably makes the root less susceptible to compression. Remember that the disc herniation material is toxic to nerves. The steroid stabilizes the membrane that surrounds the root itself- making it less susceptible to chemical contamination.
Of course, there are potential risks of steroids and they need to be discussed with your physician but the global benefits of the steroid injection cannot be underestimated. Many times, it is the only substance that can give such immediate relief and continue that relief for a longer period of time. Steroid should be thought of as a management tool for the spinal generated pain. The procedure should be simple for a skilled and meticulous physician.
Dr. Donald Corenman is committed to meeting the needs of patients in Colorado and throughout the US. For more information on epidural injections and selective nerve root blocks (diagnostic and therapeudic), please contact Dr. Donald Corenman at 888-888-5310.
Related Articles
- Lumbar Discograms
- Cervical Discograms
- Facet Blocks and Rhizotomies
- Diagnostic vs Therapeutic Injections
- Pain Diary Instructions for Spinal Injections
- Home Testing For Leg Weakness
- How to Describe Your History and Symptoms of Neck, Shoulder and Arm Pain
- How to Describe Your History and Symptoms of Lower Back and Leg Pain
- Walking (gait) Disorders
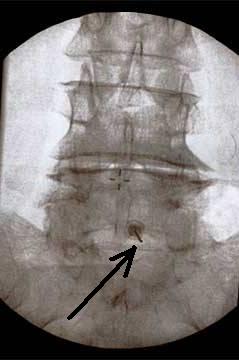
(Click to Enlarge Image) The black arrow points to the needle placed into the epidural space at the L5-S1 level.
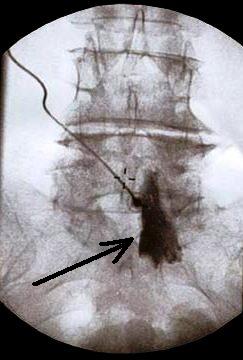
(Click to Enlarge Image) The black arrow points to the x-ray dye that fills the left side of the canal and confirms the placement of the needle tip and the ability to spread the medication in the correct location.
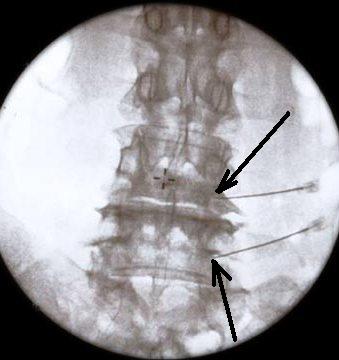
(Click to Enlarge Image) The black arrows point to the location of the needle tips for this selective nerve root block (SNRB) of both the L4 and L5 nerve roots.

(Click to Enlarge Image) The dye pattern illuminates the path of both nerves. This is called a “neurogram” and confirms that the medication to be injected will be delivered in the correct location. Notice that the dye only enters the spinal canal to the origin of each nerve from the dural sac. These are perfectly placed needles.