An Overview of Cervical Laminectomy, Laminoplasty and Posterior Cervical Fusion
Cervical laminectomy, laminoplasty and posterior cervical fusion are procedures performed in the back of the neck. The incision in the rear of the neck will expose the lamina and facets and allow the surgery to extend down into the thoracic spine. These anatomic areas have great utility for certain conditions.
The lamina is the roof of the spinal canal. The spinal canal houses the spinal cord. If there is compression of the cord, unroofing the canal will allow the spinal cord to drift backwards and give the cord more room to prevent compression. This is called a laminectomy (“ectomy” means to remove in Latin). This is a simple surgery to perform but has some consequences to understand. If the spine has developed a degenerative kyphosis (a curve backwards from the normal lordosis curve) which is not uncommon with degenerative changes causing cord compression, the laminectomy has limited value. The cord needs to be able to drift back enough from the crowded spinal canal and the abnormal curve may not let this happen.
Cervical Laminectomy & Laminoplasty
The laminoplasty is a procedure similar to the laminectomy, but instead of removing the lamina, the lamina is enlarged to allow more room for the spinal cord. The procedure is technically more demanding as the lamina must be partially cut, stretched and then fixed in its new position with a bone graft and a small titanium plate at each level. The usefulness of this procedure is similar to a laminectomy (cord compression and myelopathy) but may give more stability to the operated segments than a laminectomy can. Of course, the repaired lamina must heal in a laminoplasty and there is no healing required in a laminectomy.
In either procedure (cervical laminectomy, laminoplasty and posterior cervical fusion), there is a danger to the C5 nerve roots, not from the technical aspects of surgery but from the new displaced position of the cord. As noted above, the spinal cord should “drift” backwards with a successful laminoplasty or laminectomy. Of course, the nerve roots are attached to the spinal cord. The cord drifting back will by definition, stretch the nerve roots somewhat. The shortest and least easily stretched roots are the C5 roots that attach to the deltoid muscles (the shoulder muscles that raise and lower the humerus- the upper arm bone). Occasionally, there may be weakness of these muscles after surgery but they normally recover after a period of time. There are rare times that some weakness can be permanent.
Are you a candidate for Cervical Laminectomy, Laminoplasty or Posterior Cervical Fusion?
Would you like to consult with Dr. Corenman about your condition?
You can set up a long distance consultation to discuss your
current X-rays and/or MRIs for a clinical case review.
(Please keep reading below for more information on this treatment.)
Posterior Cervical Fusion
Posterior cervical fusion is as the name implies, fusing the back of the neck. This procedure can be used because of fracture, deformity, pseudoarthrosis (lack of successful fusion in the front of the neck- ACDF) and to extend a fusion down to the thoracic spine. Since a fusion requires immobilization to work, screws, rods and wires are typically used. Bone graft is then placed along the facets and normally, within 3 months, a solid fusion occurs.
A posterior fusion can be used in conjunction with a laminectomy to decompress the spinal cord or a foramenotomy to decompress a nerve root (see section on posterior cervical foramenotomy for further description of that procedure).
To learn more about cervical laminectomy, laminoplasty and posterior cervical fusion as a treatment option for spine related conditions, please contact Dr. Donald Corenman, spine surgeon and neck doctor offering diagnostic and surgical second opinions to patients in the USA and around the world.
Related Content
- Anterior Cervical Decompression & Fusion (ACDF)
- Artificial Disc Replacement (ADR) for Cervical Spine
- Cervical Laminectomy, Laminoplasty and Posterior Cervical Fusion
- Posterior Cervical Foramenotomy
- Myths of Laser Spine Surgery
- How to Describe Your History and Symptoms of Neck, Shoulder and Arm Pain
- Best Questions to Ask When Interviewing a Spine Surgeon or Neurosurgeon
- When to Have Neck Surgery

(Click to Enlarge Image) Preoperative lateral x-ray of the cervical spine. The black double arrow notes the reduced diameter of the spinal canal causing compression of the spinal cord.
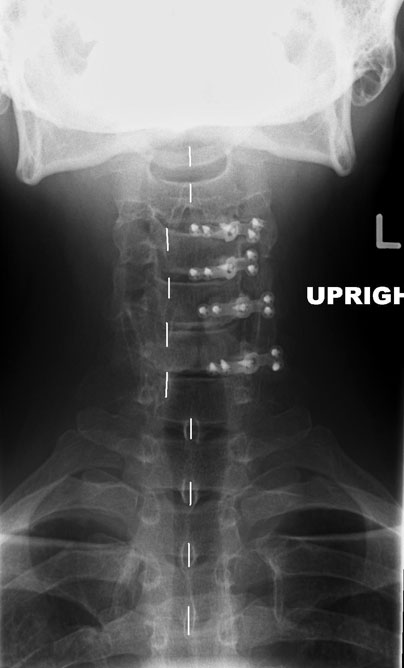
(Click to Enlarge Image) Post operative XP x-ray of the laminoplasty. Please note that the spinous processes (noted by the white lines) are “off center” in the area of surgery as the back wall of the canal that the spinous processes attach is rotated to the side to open the canal.

(Click to Enlarge Image) Post-operative lateral x-ray of the laminoplasty. The black double arrow notes the enlarged canal. Compare to the pre-operative x-ray.
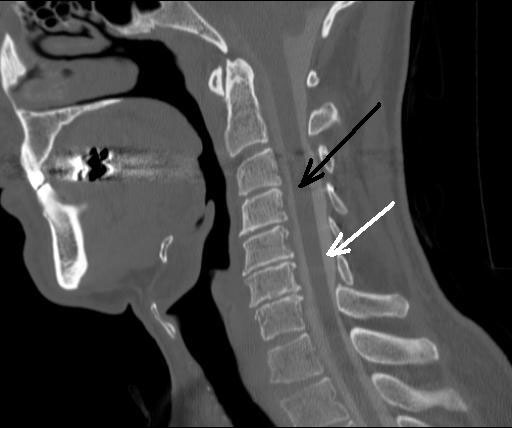
(Click to Enlarge Image) Post operative CT myelogram of the laminoplasty. The black arrow points to the spinal cord and the white arrow points to the CSF. Note that the spinal cord is surrounded by CSF which means there is no compression of the cord.