An Overview of Pars Interarticularis Fractures
and Spondylolysis in Children
Anatomy
The pars interarticularis is the bony portion of the vertebra that connects the pedicles to the inferior (lower) facets. In fact, the term “interarticularis” means the area between two articulations (joints). There are two pars interarticularis bony junctions- one on each side. The two lower joints below the pars articulate with (hook onto) the upper joints of the vertebra below.
The purpose of these lower joints is two fold. One is that these joints act like railroad tracks to guide the motion of the vertebrae above on the vertebra below. The second function of these joints is that they act as “doorstops” to prevent the vertebra above from sliding forward on the lower vertebra. The lower two vertebra (L4 and L5) sit on a ski slope pointing downhill and these intact “doorstops” prevent this slide.
In the front of the two vertebrae sits the disc. The disc is an excellent shock absorber or “bushing”. This disc is the main cushion for spinal impact. The disc however has no directional stability. Without the facets in back to protect it, the disc can twist, flex and extend, laterally bend and tilt and shear (slip forward and backwards). It is the intact facets that prevent the spine from bending in certain injurious directions.
When the connections between the facets and the pedicles are severed (pars interarticularis fractures), the disc is unprotected and can undergo motions that can cause damage. The disc is especially sensitive to rotational and shear forces, the forces that cause one vertebra to slide forward, sideways or rotate on the other. The facets prevent these forces on the disc by acting as “doorstops”.
Because the upper vertebra’s lower facets hook onto the lower vertebra’s upper facets, the intact facets restrict the shear forces of the vertebral segments. If the facets wear out (as in the case of a degenerative spondylolisthesis) or break off (as in the case of bilateral pars fractures or isthmic spondylolysis), this protection is lost. If the disc gives way and the vertebra then slips forward on the one below, this problem is called an isthmic spondylolisthesis.
It is estimated that one of every twenty children will develop pars interarticularis fractures. If these fractures occur, they normally occur between the ages of 8 and 15 years. Why are these fractures not more commonly diagnosed in this age group? Many times the child that develops new fractures will not initially complain of significant symptoms or will ignore the pain and not report it to parents, coaches and trainers.
Early Diagnosis and Potential Healing
If the fractures are diagnosed early in childhood, the pediatrician is the physician that normally uncovers the fractures. Many injured children however never become diagnosed. This section deals with what to do if these fractures are diagnosed early when the child still has a chance to heal and the disc has not been injured.
In general, children generally have very good bone fracture healing potential. The pars interarticularis fractures however are the one set of fractures in particular that are resistant to healing. There are three reasons for this. One is that the surface area of these fractures is very small. Bone fractures heal best with large surface areas and the surface area of this fracture is smaller than some of the smallest bones in the hand.
Bone also has better healing potential when large cancellous surface areas are exposed. Cancellous bone is the “spongy bone” inside the hard cortical bone and has many bone generating cells. Unfortunately, the pars interarticularis has almost no cancellous bone.
The third problem is that this area of the spine has some of the greatest motion and shear forces acting on it, This fact is one of the main reasons the bone fractured in the first place. Getting an active child or teenager to rest this area is almost an act of God. A brace can slow a child down but will not immobilize the area and healing bone cells do not respond well to motion.
In the typical bilateral pars fractures, healing without a brace and without reduced activity has a very poor repair rate. Healing with a brace and three to six months of reduced activity has a success rate of about 50%. The chance of re-fracture is not know at this time but children with healed fractures can occasionally re-fracture if they go back to their previous level and type of activity.
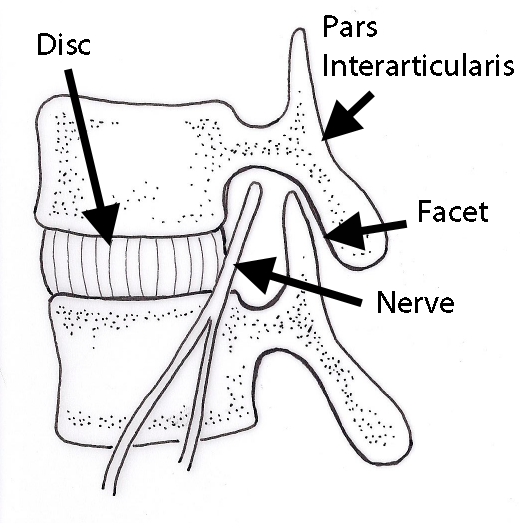
(Click to Enlarge Image) Illustration of pars interarticularis.

(Click to Enlarge Image) CT scan of pars fracture of L5. White arrow points to fracture. Thisadolescent had 4 months in brace and continued to have pain upon return to activity.

(Click to Enlarge Image) CT axial scan of L5 pars fracture. White arrows point to fractures of pars interarticularis.
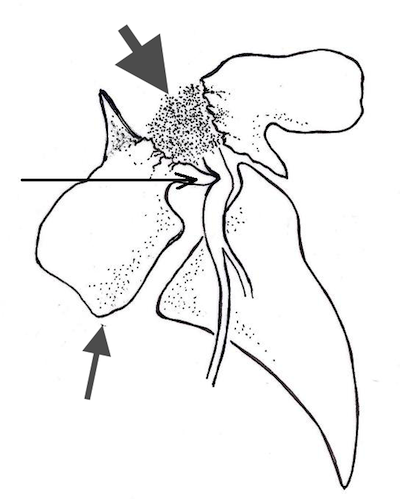
(Click to Enlarge Image) Illustration of Isthmic Spondylolysis. Thin arrowpoints to bone spur compressing the nerve. Medium arrow points to the slipof L5 on the sacrum. Thick arrow points to the non-healed fracturepannus.

(Click to Enlarge Image) Isthmic Spondylolysis. Note the slipof the L5 vertebra on the sacrum. This is the endpoint of degenerativewear resulting initially from an undiagnosed spondylolysis when thepatient was a child.
Is your child suffering from symptoms of a pars interarticularis fracture?
Would you like to consult with Dr. Corenman about your condition?
You can set up a long distance consultation to discuss your
current X-rays and/or MRIs for a clinical case review.
(Please keep reading below for more information on this condition.)
Unilateral (One Sided) Pars Interarticularis Fractures
Although it is uncommon for only one side of the pars interarticularis to fracture, unilateral fractures do occur. If a unilateral pars fracture does arise, the opposite pars will be placed under more stress and therefore will hypertrophy (lay down more bone-Wolfe’s Law) to resist the greater forces placed upon it. If the fractured side does not heal, the greater bone mass of the opposite side may allow an individual who has a unilateral pars fracture to live with it comfortably. However, the unilateral break may create enough stress on the opposite side to eventually fracture it also.
The unilateral pars fracture has a much better chance of healing with rest and bracing. Think of the vertebra and both pars interarticularis as a ring. If only one break of the ring occurs, the ring still has some torsional rigidity. If there are two breaks, the ring is broken in half and has no rigidity. A recently diagnosed one-sided (unilateral) break allowed three months of bracing and rest will normally heal.
Healing potential and resolution can be assessed by MRI, X-rays, bone scan and CT scan. There are particular appearances that may indicate an effort by the body to heal the fracture and conversely, a noted lack of healing potential.
The unilateral pars interarticularis fracture needs to be differentiated from a facet fracture. If the fracture line starts at the pars interarticularis but descends obliquely instead of normally traversing across the pars, this fault line can fracture off the entire facet. A facet fracture will not heal. The CT scan is the only useful tool to diagnose this injury.
Non-Healed Fractures and Altered Biomechanics
What is the future of the spine in the adolescent with bilateral pars fractures that do not heal? If both pars are fractured, the biomechanics of the spine changes. There is more stress placed upon the disc and the entire spine can slip forward (isthmic spondylolisthesis– see separate section on this website). This leads to disc tears and degenerative changes of the disc. Some patients develop lower back pain and even leg pain if a pedicular bone spur develops. To prevent degenerative changes from occurring, there is mounting evidence that the pars fractures need to be surgically repaired.
Please see section on surgical pars repair on this website for further information.
For more information on spondylolysis in children, or to discuss treatment options for a pars interarticularis fracture, please contact Dr. Donald Corenman, back doctor and spine specialist in the Vail, Aspen, Denver and Grand Junction, Colorado area.
Related Content
- When to Have Lower Back Surgery
- Causes of Lower Back Pain
- Normal Spinal Alignment
- Lumbar Spinal Alignment
- How to Describe Your History and Symptoms of Lower Back and Leg Pain
- Best Questions to Ask When Interviewing a Spine Surgeon or Neurosurgeon
- Degenerative Spondylolisthesis
- Isolated Disc Resorption-Lumbar Spine (IDR)
- Lumbar Spinal Stenosis (Central Stenosis)