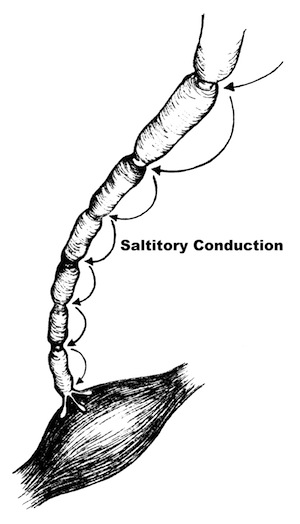
(Click to Enlarge Image)
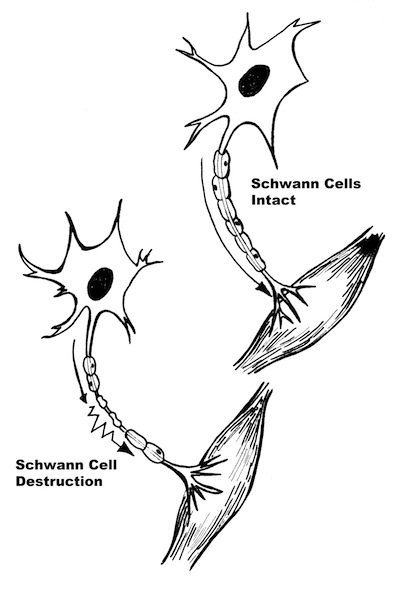
(Click to Enlarge Image) Schwann cell nerve injury and conduction block.
An Overview of Nerve Entrapment Syndromes
All of the syndromes noted below involve trapping of a peripheral nerve in a tunnel.
• Meralgia Paresthetica (Lateral Femoral Cutaneous Nerve Entrapment)
• Peroneal Nerve at Fibular Head Entrapment
These peripheral nerves are different from the nerves in the spinal canal (the radicular nerves) due to their “protective armor”, the epineurium and perineurium. This protective sheath makes the nerve less vulnerable to injury than the spinal nerves. Nonetheless, these nerves can be injured by stretch, impact and compression.
All of these nerve entrapment syndromes are very similar in their pathology (the basic disorder that causes the problem). This pathology is compression of the nerve by a bone or tendon. The difference in each disorder is the nerve distribution (where the nerve travels and what it does) and whether this nerve contains only sensory nerves, only motor nerves or a combination of the two.
Thoracic outlet syndrome (a shoulder nerve compression condition) is somewhat similar to all these entrapment syndromes but has some different qualities. The brachial plexus, the set of nerves which are compressed in thoracic outlet syndrome, contains all the nerves traveling to and from the arm. Thoracic outlet syndrome is discussed as a separate topic on this website.
You can read about the specifics of what causes the microscopic damage to a nerve in the separate topic “Nerve Injuries and Recovery” on this website.
If the compressed nerve has strictly a pure sensory distribution, no motor weakness will be present and therefore no atrophy can occur. Atrophy only occurs when the muscle belly shrinks due to a lack of nerve supply.
The only pure sensory nerve in the list above is the Lateral Femoral Cutaneous Nerve. This nerve supplies only pain fibers and sensation to the anterior and lateral thigh. Since there is no muscle that is involved with this nerve, there is no neurological weakness with this condition called Meralgia Paresthetica.
However, pain inhibition can cause temporary muscle weakness in certain leg positions. This is not true muscle weakness but an actual subconscious reflex to prevent pain from occurring by subconsciously refusing to contract the muscle for fear of pain.
We will first discuss the general symptoms that can occur with peripheral nerve compression.
Sensory Symptoms
With all these syndromes, the nerve becomes compressed and then can become injured. As pressure increases on the nerve, the blood flow decreases. This causes nerve malfunction such as conduction loss and unintended conduction called ectopic stimuli. Loss of conduction means the nerve will not convey messages to the brain from the skin. This loss of sensation is obviously described as “numbness”.
Injury can also cause conduction to occur even when the nerve is not stimulated (ectopic stimulation). This is like a short circuit in doorbell wiring making the doorbell ring when no one is at the door. This sensation is noted by the patient as pain, paresthesias (pins and needles) as well as bizarre sensations (ants crawling or cold water splashing on the skin).
The continued crush injury can also injure the myelin sheath, the “insulation” of the nerve. This can be more of a permanent injury. Myelin sheath injuries can heal but this healing takes between 8-14 weeks for recovery.
With compression of the nerve, increased “pins and needles” (paresthesias) typically occur. Electric shock sensations (Tinel’s sign) that “zing” down the nerve then can occur. Abnormal spontaneous hot and cold sensations can develop in the distribution of the nerve
With chronic injury, fluid collects in the space that the nerve occupies and the nerve itself can swell, increasing the intensity of the symptoms. Continued nerve injury produces increased swelling and can induce pain. Burning sensation can occur when the nerve develops permanent injury. The pain can worsen and spread. Pain tends to be worse with activity and is relieved by rest but continuous pain can occur with chronic injury.
Motor Symptoms
For those nerves that contain motor fibers, motor strength loss typically occurs gradually. There are rare circumstances however where the entire muscle group can fail all at once. For instance, in the leg with peroneal neuropathy, this might manifest as foot drop, the inability to hold the foot up when walking. With foot drop, the foot will slap on the ground or even “catch”: the ground when the foot swings through when walking. In the case of carpel tunnel syndrome, grasp can become difficult with the effect of the feeling of clumsiness (inadvertently dropping objects).
As small muscles lose their nerve supply they can create a “cramping feeling”. Cramping can be an indication of weakness but other non-related disorders can also cause cramping.
Are you suffering from symptoms of a nerve entrapment syndrome?
Would you like to consult with Dr. Corenman about your condition?
You can set up a long distance consultation to discuss your
current X-rays and/or MRIs for a clinical case review.
(Please keep reading below for more information on this condition.)
Causes of Nerve Entrapment Syndromes
Most entrapment syndromes are caused by mechanical and genetic problems. Genetics have to do with the size of the tunnel these nerves travel in. Some people have congenitally smaller tunnels and with aging, previous injury, degeneration (bone spurs) and inflammation, these tunnels become crowded. Mechanically, overuse syndrome can cause tendons to swell (tendonitis and synovitis) and crowd out the nerve.
There are genetic and metabolic disease processes that can contribute to nerve malfunction. These processes may increase the swelling (crowding) of the tunnel or make the nerve itself more sensitive. These disorders include rheumatoid arthritis, hypothyroidism, pregnancy, diabetes, acromegaly (too much human growth hormone) and CMT syndrome (Charcot Marie Tooth syndrome-a genetic condition).
Specific Nerve Entrapment Syndromes
Click on any condition below to see the specifics of this condition:
• Carpel Tunnel Syndrome
• Cubital Tunnel Syndrome
• Meralgia Paresthetica (Lateral Femoral Cutaneous Nerve Entrapment)
• Piriformis Syndrome
• Peroneal Nerve at Fibular Head Entrapment
• Tarsal Tunnel Syndrome
For additional information on nerve entrapment syndromes, or to discuss nerve entrapment compression, please contact the practice of Dr. Donald Corenman, spine specialist and back doctor offering diagnostic and surgical second opinions to patients in the USA and around the world.