Stingers and Burners Overview
Stingers and burners are really two names for the same injury; a stretch of the brachial plexus. The brachial plexus is the compilation of the five separate nerves roots that originate in the neck and begins when the radicular nerves leave the neck through the foramen (the holes in the spinal vertebra that these nerves begin from).
These nerves (C5 through T1) originate from the C4-5 interval (C5 nerve) and continue to originate from T1-2 (the T1 nerve). When these nerves exit the neck, they “perform a dance” where the nerves join, blend, branch and then separate. These now mixed nerves transfer through the front of the chest under the collarbone and descend down into the arms.
All sensation and motion from the shoulders to the hands originate from these nerves.
Mechanically, the nerves are secured onto the spinal cord and solidly attach into the upper arm and hands. They act as cables and are fixated by these two separate locations. An abnormal force on the neck and arm can stretch them and nerves do not like to be stretched.
The upper nerves (C5 and C6) have the potential to be stretched more than the lower ones due to their upper location (more motion) and shorter length. This shorter length makes these nerves more susceptible to stretch injury as a shorter nerve has less ability to tolerate stretch.
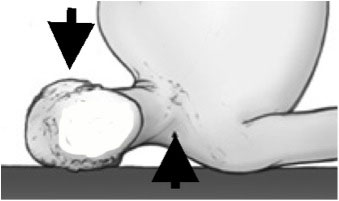
(Click to Enlarge Image) When the head is laterally flexed (bent to the side) and forward flexed (chin to chest) and the shoulder is depressed (pushed down), this is the perfect combination for this stretch injury, the “stinger”. Nerves are like cables that travel over a pulley (the shoulder). Since these nerves are rigidly fixed to the neck and the arm, when the neck is forced to the opposite side and the shoulder is depressed down, they are severely stretched.
Are you suffering from symptoms of a brachial plexus injury?
Would you like to consult with Dr. Corenman about your condition?
You can set up a long distance consultation to discuss your
current X-rays and/or MRIs for a clinical case review.
(Please keep reading below for more information on this condition.)
What is the Nerve Injury?
When the head is laterally flexed (bent to the side) and forward flexed (chin to chest) and the shoulder is depressed (pushed down), this is the perfect combination for this stretch injury, the “stinger”. Nerves are like cables that travel over a pulley (the shoulder). Since these nerves are rigidly fixed to the neck and the arm, when the neck is forced to the opposite side and the shoulder is depressed down, they are severely stretched.
If a nerve is stretched, it may simply recoil to its original length when the stretching force is released. If the stretch is substantial, the nerve may completely snap, similar to the stretch and snap of a rubber band. In general, a nerve can stretch about 6% of its length without injury. Stretching between 6 and 15% will cause temporary damage to the nerve. A stretch of more than 15% of the nerve’s length will cause irreversible damage. No one has yet studied what happens to a nerve that has multiple stretch injuries in this 6-15% zone but clinically, some patients have permanent symptoms with multiple stretch injuries (stingers).
In a brachial plexus injury, when the nerve cell is injured, generally the membrane of the nerve can be “stunned” (a temporary “concussion” to the nerve). The nerve can also suffer reversible or irreversible damage. The insulation (myelin sheath) can also be damaged. When the nerve cell membrane is “stunned” or damaged, the signal can be blocked which prevents the message from continuing down the nerve. The opposite effect can also occur. Injury to the membrane can cause “leaks” or ions to flow into the nerve at the wrong time, triggering an unintended impulse called an ectopic impulse.
This temporary block of a nerve membrane prevents the message from traveling up to the brain or down the nerve from the brain to the muscle. This would result in numbness of the area served by the nerve and weakness of the muscle supplied by the injured nerve.
What are the Symptoms of Stingers and Burners?
Symptoms are exactly as this disorder is named, burning or stinging down the arm into the hand. This sensation can feel like electrical bolts of lightening.
The arm can feel “dead”. An injured player might return to the bench with the arm hanging by his or her side or this individual might protect their arm with the other hand.
Symptoms typically resolve within minutes of the stretch injury. Repeat injuries can be cumulative which both increase the chance for another injury and could increase the permanent nature of the injury. Multiple injuries could lead to chronic paresthesias (pins and needles), numbness and weakness.
Who gets Stingers and Burners?
Participants in contact sports and sports that allow the participant to travel at a high rate of speed without protection can lead to this injury. Football players are the prototypical athletes who are susceptible to stingers and burners but soccer players and rugby contestants quite commonly suffer from stingers. Skiers and boarders who hit a tree, mountain bikers who impact terrain while descending or surfers with a fall onto a coral reef can injure their brachial plexus.
Treatment of Stingers and Burners
Treatment of the brachial plexus injury is initially discontinuation of play and restriction of motion of the injured extremity. Possibly a sling might be considered if the extremity is very weak. Analgesics are used for pain and rest is the main consideration. If the arm does not regain strength and sensation quickly, other diagnoses need to be considered.
Return to Play Following a Brachial Plexus Injury
Return to play depends upon full resolution of all symptoms and a physical examination that is normal. Persistent symptoms in athletes signal that they should not be allowed to participate in further competition until complete resolution of their symptoms has occurred.
If the athlete has neck stiffness but no longer has arms symptoms, this symptom needs to be addressed to make sure there are no cervical injuries present.
Differential Diagnosis
The brachial plexus injury needs to be differentiated from a central cord injury. Central cord injury is a spinal cord injury that produces temporary paralysis that may last only seconds. The differential is that stinger symptoms are found in only one arm and central cord syndrome is found in both upper extremities. Central cord syndrome is also known and “burning hands syndrome” as the back of the hands will “feel on fire”.
The mechanism of the central cord syndrome is an extension injury of the head (bending the head backwards) in the presence of a narrowed spinal canal. This extension motion will narrow the spinal canal and if the canal is already narrowed, will “pinch” the cord. See central cord syndrome on this website for a more detailed description of this disorder.
If there are symptoms on both sides, this injury is not a stinger or a burner.
Herniated discs can occasionally mimic a stinger as there will be pain and numbness in one arm. A careful history and physical will lead to the discovery of single nerve involvement, which is not typical of a stinger and burner. Herniated disc symptoms generally will not quickly resolve on the field, which means the competitor will not return to immediate play. Motor testing on the bench is sometimes necessary as pain might not start immediately after a herniated disc but weakness will. Hopefully, this individual will then see a spine expert for appropriate diagnosis. An EMG (electrical nerve test) could be considered after three weeks of symptoms that do not resolve in the face of continued weakness.
Although very rare, stingers need to be differentially diagnosed from nerve avulsion injuries. Nerve avulsions (tearing of the nerve) generally occur with great force or impact mechanisms. I had a patient who was traveling on a motorcycle at 70 mph at night and hit a moose. The force was so great that he actually avulsed his nerves (tore them apart in the shoulder) and had significant weakness of his arm. This should not happen to a contact sports player but I have seen this injury also in a skier vs. tree impact (the tree always wins).
For more resources on stingers and burners, or to determine the appropriate treatment option for a brachial plexus injury, please contact the office of Dr. Donald Corenman, spine specialist and back doctor serving the Vail, Aspen, Denver and Grand Junction, Colorado communities.